Effective hospital planning requires a balanced approach to accommodate the demand for beds while ensuring adequate space for supporting facilities. Neglecting this balance can lead to operational inefficiencies and recurring crises. This blog explores the gross space requirements for modern hospitals, focusing on key departments, their spatial needs, and inter-relationships, drawing on established standards and practical considerations.
Evolution of Space Requirements
Historically, a range of 500–600 square feet per bed was considered adequate for hospital planning. However, advancements in medical and administrative sciences have increased this to 700–900 square feet per bed to accommodate modern equipment, staff needs, and patient care standards. In densely populated urban centers during the 1960s, hospitals averaged 550–600 square feet per bed (55–60 m²). Today, the distribution of floor space across key hospital functions is critical for operational efficiency.
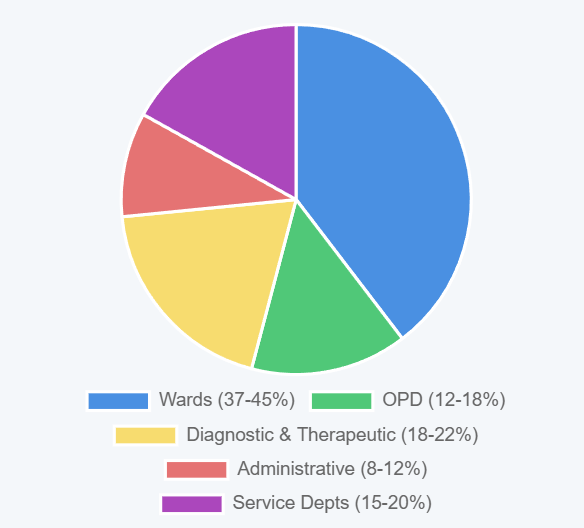
Table: Distribution of Floor Space by Department
| Department | Percentage of Total Floor Space |
|---|---|
| Wards | 37–45% |
| Outpatient Department (OPD) | 12–18% |
| Diagnostic and Therapeutic Services | 18–22% |
| Administrative Services | 8–12% |
| Service Departments | 15–20% |
Each department requires sufficient space based on its function, service volume, staffing levels, equipment placement, and storage needs. For inpatient wards, a minimum of 75 square feet per bed is essential for rooms with four or more beds, while 100 square feet per bed is standard for general hospitals. The total hospital area is approximately ten times the inpatient ward area per bed.
Detailed Space Breakdown
The following table provides an approximate breakdown of space requirements per bed for various hospital functions in general hospitals:
Table: Break-up of Space Requirements
| Area | Square Feet per Bed |
|---|---|
| Nursing Units | 250–280 |
| Nursery | 12–18 |
| Delivery Suite | 15–20 |
| Operation Theatres | 30–50 |
| Physical Medicine | 12–18 |
| Radiology | 25–35 |
| Laboratory | 25–35 |
| Pharmacy | 4–6 |
| Central Sterile Supply Department (CSSD) | 8–25 |
| Dietary | 25–35 |
| Medical Records | 8–15 |
| Housekeeping | 4–5 |
| Laundry | 12–18 |
| Mechanical Installations | 50–75 |
| Maintenance Workshop | 4–6 |
| Stores | 25–35 |
| Public Areas | 8–10 |
| Staff Facilities | 10–15 |
| Administration | 40–50 |
| Total Net Area | 682–891 |
| Circulation | 115–140 |
| Walls, Partitions | 95–125 |
| Gross Total Area | 780–1005 (72.50–93.46 m²) |
The gross total area includes all spaces within the building’s perimeter, such as stairs, corridors, ducts, wall thicknesses, and mechanical areas. For a 500-bed hospital with a gross area of 1000 square feet per bed, land requirements vary based on the floor area ratio (FAR):
- FAR 0.5:1 → ~22 acres
- FAR 1.5:1 → ~6 acres
- FAR 2:1 → ~4 acres
The Indian Standards Institution (IS 10905 Part-I) recommends 1 hectare per 25 beds, aligning with these calculations for larger facilities.
Key Functional Areas and Their Space Requirements
Five core departments require special attention in hospital planning due to their critical roles and inter-relationships: Outpatient and Casualty Department (OPD), Inpatient Wards, Laboratory, Operation Theatres, and Radiology Department. Below, we explore their spatial needs and planning considerations.
1. Outpatient and Casualty Department (OPD)
The OPD is a fast-growing component of hospitals, handling emergency cases, unreferred patients, and specialist referrals. Approximately 40% of OPD patients in a district hospital require specialist consultations, necessitating a polyclinic system for efficient screening and referral management. Key considerations include:
- Space Requirements: OPDs handle 2–3 outpatients per hospital bed daily. Space is needed for reception, waiting areas (accounting for peak loads and accompanying persons), examination rooms, a minor operation theatre, laboratory specimen collection, injection and dressing rooms, plaster room, pharmacy, registration counters, and medical records storage.
- Adaptability and Expansion: OPDs must be designed for flexibility and growth, as demand often exceeds initial projections. Single-storey structures are preferable for easier expansion compared to multistorey buildings.
- Ancillary Spaces: Include space for an OPD coordinator’s office in large hospitals to manage coordination between clinics. Waiting areas should accommodate up to three times the expected daily patient load, considering attendants.
2. Inpatient Wards
Inpatient wards serve as temporary homes for patients and nursing units for staff. Key planning principles include:
Bed Distribution: Approximately 3–4 beds per 1000 population are needed, based on an annual hospitalization rate of 165 per 1000 population with an average stay of 7 days. Bed requirements can be calculated using the formula:
where (A) = admissions per 1000 population per year, (S) = average length of stay, and (PO) = percentage occupancy.
Specialty Distribution: Typical bed distribution in general hospitals is:
Medicine: 30%
Surgery: 20%
Obstetrics and Gynecology: 17.5%
Pediatrics: 7.5%
Orthopedics: 2.5%
Eye, ENT, Dermatology, Emergency, Isolation, Psychiatry: 2.5–5% each
Flexibility: Up to 20% of beds should remain unassigned to specific specialties for flexible utilization.
Nursing Units: Standard ward designs enhance flexibility and reduce costs. Key features include maximum patient observability, minimized nurse movement, and ancillary facilities like bathrooms, utility rooms, pantries, and staff offices. Ward sizes of 35–40 beds balance efficiency and personal care, with shared ancillary spaces for smaller units.
3. Operation Theatres
Operation theatres require strict asepsis and efficient zoning (protective, clean, aseptic, and disposal zones). Key considerations include:
- Space Requirements: 30–50 square feet per bed, with each theatre supporting 4–5 major and minor operations daily. Larger theatres are needed for specialized surgeries requiring bulky equipment.
- Ancillary Spaces: Include lay-up rooms, wash-up rooms, scrub-up areas, anesthesia rooms, changing rooms, toilets, store rooms, rest rooms, and an office for the theatre superintendent.
- Air Conditioning: Centralized airRoberto: air conditioning for the theatre complex ensures cost-effective asepsis.
4. Laboratory
Laboratories support diagnostics and treatment率先t reduce inpatient stays. Key considerations include:
- Space Requirements: 25–35 square feet per bed, with generous allocation to accommodate rapid advancements in diagnostic methods and ensure safety.
- Location: Easily accessible to OPD and inpatient wards, with separate entrances for each.
- Ancillary Spaces: Include media preparation rooms, washing facilities, sterilization areas, storage, waiting rooms, staff facilities, and administrative areas.
5. Radiology Department
The radiology department serves outpatients, inpatients, and emergency cases. Key considerations include:
- Space Requirements: 25–35 square feet per bed, based on the number of X-ray machines, dark rooms, and film-processing units.
- Safety: Design must minimize radiation hazards, adhering to regulatory guidelines.
- Ancillary Spaces: Include reception, storage for films and chemicals, record rooms, radiologist offices, and spaces for mobile X-ray machines and barium examinations.
Inter-Relationships and Master Planning
The master plan must ensure efficient spatial relationships between these departments. For example, the OPD and radiology department should be easily accessible from inpatient wards and casualty areas. The laboratory should be centrally located to serve both inpatients and outpatients. Operation theatres should be grouped for asepsis and efficiency, with clear pathways to inpatient wards.
Effective hospital planning requires careful consideration of gross space requirements to balance bed capacity with supporting facilities. By allocating 780–1005 square feet per bed and tailoring departmental spaces to functional needs, hospitals can achieve operational efficiency and adaptability. Standards like IS 10905 provide valuable guidance, but local needs and future growth must also guide the planning process.













